

Why Physicians Underestimate Their Networks
You built your network over fifteen years of training and practice without noticing - and never looked back to see what it had become.


A handful of years ago, I was quietly searching online job boards after the workday was done, looking for a change. I talked to recruiters, browsed postings, and touched base with colleagues at other institutions - the usual methods. None of it led anywhere interesting.
The way I learned about my next opportunity was from talking to a physician who also served with me on a statewide quality and safety committee. It just came up in casual conversation at the beginning of one of the meetings, when people were just settling in, and I asked him where he practiced and how he liked it. It turned out that there was a whole different type of practice structure in my geographic area that I had no idea existed - a multispecialty outpatient practice, one which would allow me to read similar types of cases and perform similar procedures compared to my current private practice, but with different workplace settings and hours, as well as a few other key differences. Long story short, I ended up joining his practice a little while later - Atrius Health - and it’s the exact one that I practice at today.
This led me to the realization that a physician could spend a lot of time searching online for the right job, role, or opportunity, without realizing that the best opportunities often travel through networks of people - human one-to-one connections - not online databases.
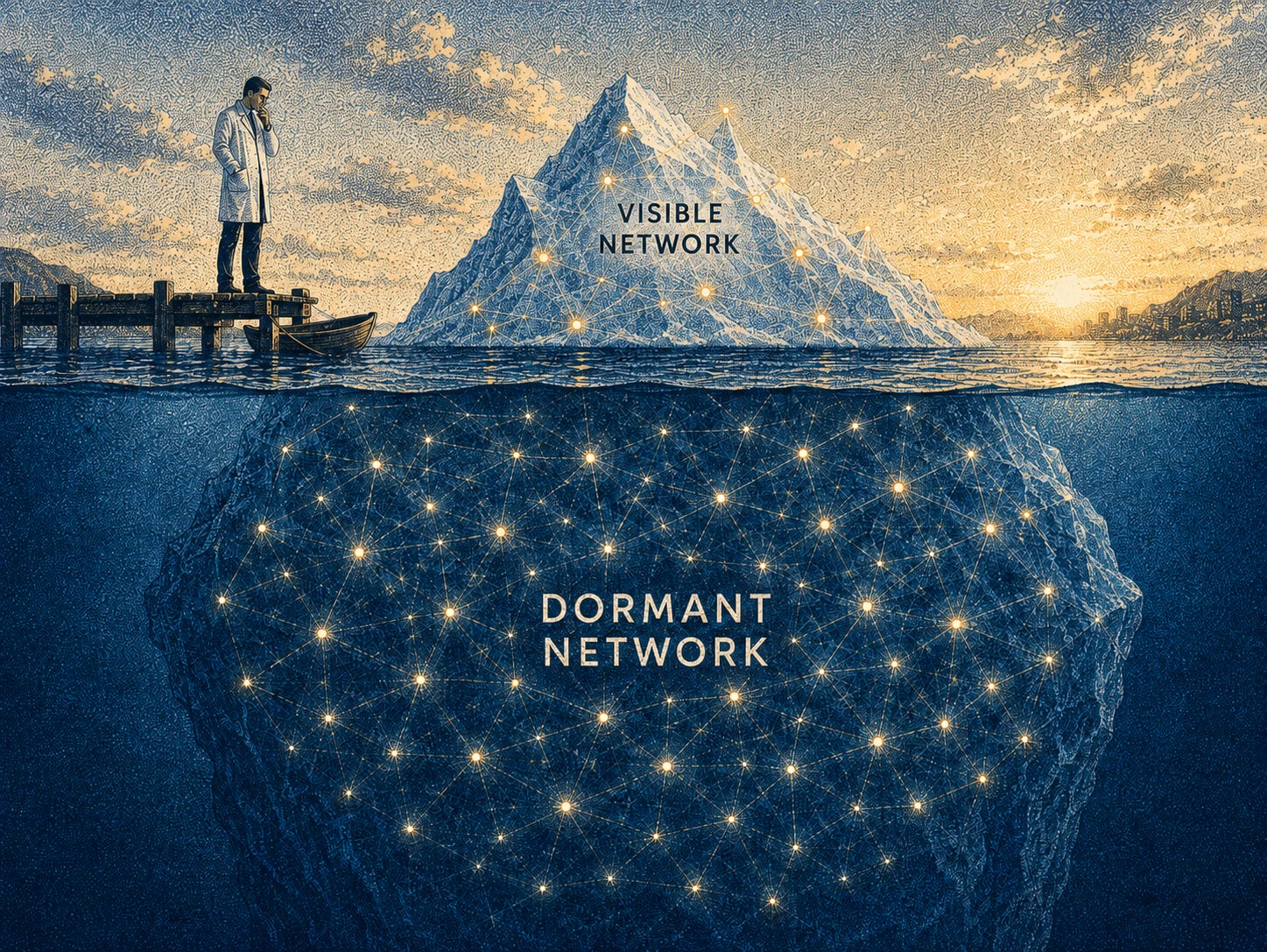
This revealed a truth that I understand today. Physicians often underappreciate the multifaceted relationships they currently have and the ways in which they can activate them. They tend to think about their network the way you’d think about an iceberg: the visible part - the referring physicians, the current colleagues, the people you’d call this week - is all they see. But below the waterline sits something much larger and almost entirely unappreciated: the full decade or more of medical school classmates, former co-residents and fellows, former attendings, conference contacts, and colleagues who left clinical medicine entirely and now serve inside health systems, venture, or industry. Most physicians can describe the visible part of the iceberg in detail but haven’t mapped the rest. The better way to think of the network is as a wide system of context, trust, and visibility that can allow opportunities to come to them.
Many physicians get really uncomfortable with the word ‘network’ or ‘networking’, and for good reason. But it’s important to understand that the network is really a set of relationships where information, introductions, reputation, and opportunities can travel, not merely a pool of people from which to extract favors when they’re needed. This network includes immediate strong ties, weak ties, and adjacent and tangential ties. Importantly, it’s not just about who you know but also who knows you - what do other people know you for? When your name is mentioned, what comes to mind for people? What do they think that you’re capable of, what do they think that you’re curious about, and what do they think that you spend your time on? Network leverage starts to form when people can connect your abilities to a specific opportunity.
The network shouldn’t be thought about as something that’s directly related to your popularity or how well known you are on social media, or even if you’re constantly visible or not. We should move towards thinking about the network as a source of quality connections where there’s some type of context, trust, and a reason to re-engage down the line. In this way, the network doesn’t get conceptualized as a promotional tool, but something in which there’s a mutual exchange of value and a sharing of curiosity.
And it’s often the most distant connections - the ones you’d be tempted to discount - that have the most potential opportunity. The classmate you haven’t spoken to in ages, now a VP at a health system, connects you to a world your immediate colleagues simply can’t. Research on professional networks consistently shows that these dormant, weak ties are disproportionately valuable precisely because they bring you into rooms your inner circle never touches.
Structural reasons why physicians tend to underestimate their networks
One central reason is that the training rewards competence and adherence to rules, more than visibility and network building. Clinical training, after all, rewards individual excellence: you’re evaluated by your knowledge and judgment, and not necessarily by the deliberate cultivation of your network. Another reason is that many physicians are at an inherent disadvantage if they spend most of their time inside their institutional walls and they don’t spread their message more broadly at conferences, other speaking events, or online. If you have an excellent reputation locally, that doesn’t necessarily translate to a wider network where people may understand your credibility and skills.
Also, making an ask (from a networking perspective) can feel uncomfortable. This is because physicians are used to a position of authority and being the ones who are being asked. And so it can sometimes feel uncomfortable to project the ambition or desire for a bigger path if one reaches out to their network. Physicians also tend to be more to themselves as opposed to more broadly visible. As they may reflexively guard against self-promotion, they could unintentionally keep their budding interests and skills more quiet.
Finally, the significant busyness of most practicing clinicians can erode relationships that have formed over time. When your calendar is completely full and you gradually lose touch with colleagues that you trained with or you practiced with in the past, the opportunities that used to trickle in can slow, since no one is kept up to date on what’s happening in your life. Maintaining relationships takes time, which can be in genuine short supply as a busy physician.
Most physicians already hold several network assets that have quietly gone dark from underuse.
One of the most valuable of these assets is trust and credibility. As a physician, people generally believe you’re competent, serious, and worthy. This is hard for anyone in society to generate, and physicians already tend to have this at baseline. Another inherent advantage is proximity to different opportunities, many of which are not widely advertised. They move through trusted networks first.
Another asset is your context. People will recognize your specialty, where you practice, the prestige and reputation that goes along with it, what your judgment tends to be, and also what interests you have been vocal about in the past. This type of context helps people understand what opportunities to send your way.
Another network asset is distribution, where your network can help you spread the word about important initiatives that you’re working on by forwarding your writing or bringing up your name in the right circles. Finally, another key asset is translation, where people in healthcare-adjacent fields can translate your credibility into advisory, startup, consulting, AI, or leadership opportunities.
Something even more fundamental exists however that most physicians don’t consciously think about: the trust multiplier. Physician outreach to another physician - or even to an industry leader or founder - starts from a credibility baseline that a cold contact just doesn’t have. The shared training, the shared stakes, and the credential itself all silently vouch for you before you’ve said anything. A peer-to-peer message from one physician to another gets answered at rates most professional outreach doesn’t hit, not because of communication prowess, but because of what that white coat signals.
This makes a difference because the trust multiplier exists specifically because of the clinical identity. The network isn’t a separate skill unrelated to medicine - it’s a downstream byproduct of the clinical credential. Every year of training and practice deposited trust into the bank of these relationships, and that trust is there, waiting to be seen and used. This turns “you have more contacts than you remember” from a pep talk into a legitimate leverage argument.
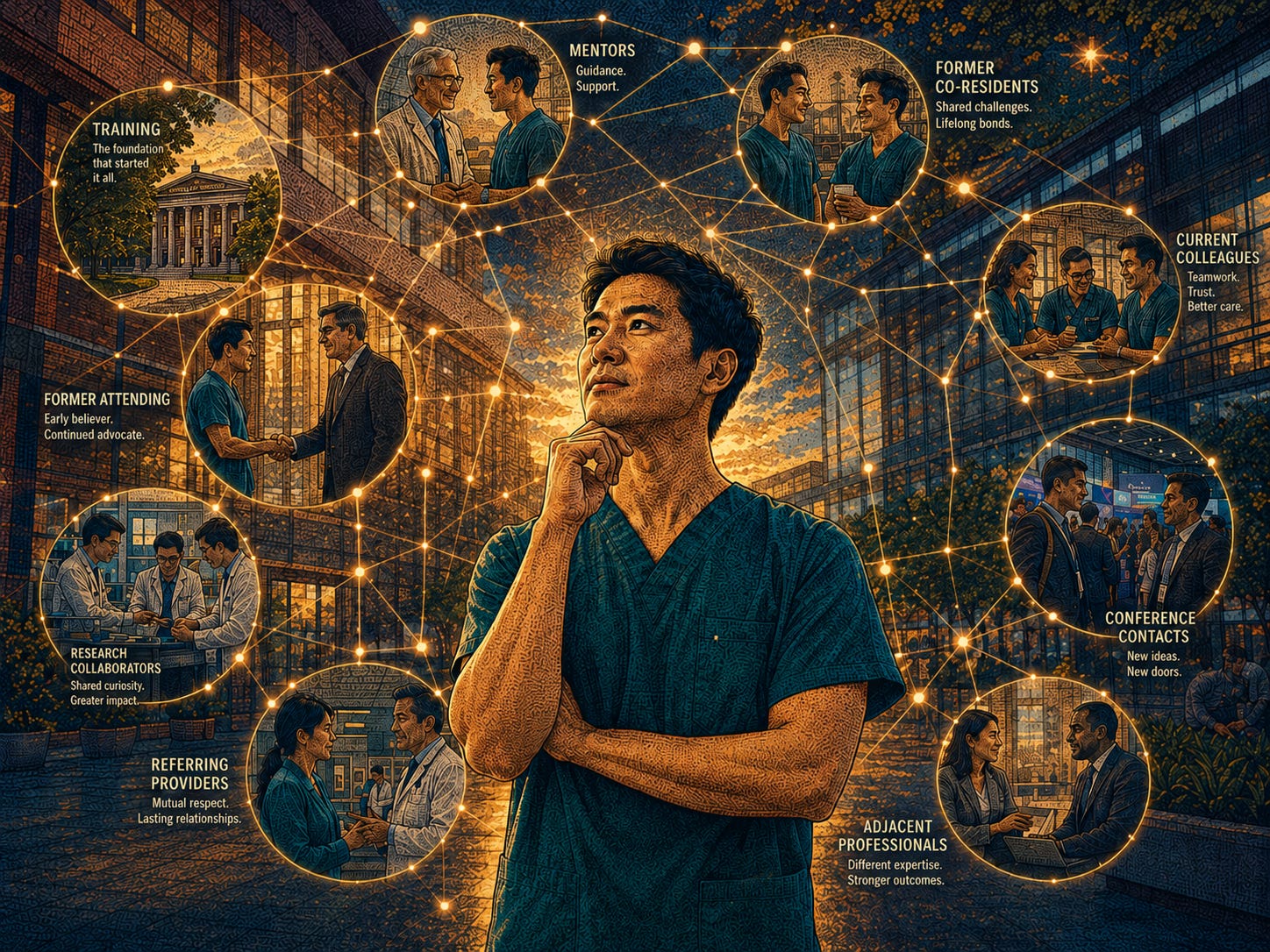
Your network is more nuanced than a single entity - you actually have several, each creating different types of opportunity. Your clinical peers - colleagues, referring physicians, multidisciplinary tumor board peers - carry the strongest trust, but the least expansion potential. Your training network, including medical school classmates, former co-residents and fellows, and mentors, is often dormant but emotionally durable, and the easiest to reactivate with a single message. Your institutional network - administrators, leadership teams, and committee members - create internal leverage. And then there are two networks most physicians barely think about: the adjacent ecosystem of investors, consultants, founders, and AI builders who are healthcare-adjacent, and the audience and community network of readers, subscribers, and online connections where platform leverage and network leverage merge and integrate.
Examples of the Networks in Practice
These multiple networks can work together in the following way, with the end result being that your credibility travels to someone distant from you.
First, it could start with you writing on a subject of importance to you, such as your views on the healthcare workforce crisis. This writing could then be noticed by someone who makes the mental link between that problem and your opinions and potential solutions. When that person later on has a subsequent conversation about that very same issue, they think about you and bring your name up. This then transfers your credibility to a new opportunity.
And the subsequent time that you write and send a signal out there, it becomes easier for it to transfer because your network now understands a little bit better about what to listen for.
So the initial writing created that signal telling your network what you’re thinking about before you’ve ever asked for anything. The later conversations create specificity about a particular opportunity - where your credibility and skill can transfer.
These introductions over time increase the number of people who know you and can imagine an opportunity for you. Your reputation and credibility compound when different people repeat the same ideas and phrases about you. Ultimately, as long as you’re known for something valuable by the right people, your network leverage is doing its job; it’s not necessary to be known by everyone everywhere.
Practical Implementation
Here’s a useful exercise to try in a single sitting - which should take fifteen minutes and a piece of paper. Write down five names per bucket across these five categories:
Clinical peers who have a high opinion of you
Former physician contacts from training who would remember you favorably
People who’ve seen you teach, create something, lead, advise, or solve a problem
Adjacent professionals from outside your clinical practice
People who you would just enjoy reconnecting with just for its own sake
Take that list in front of you, and notice three things about it:
Do they know what I’m currently working on, and where I hope to go with it?
What could I offer them that’s of value - any introduction, information, opportunity, or encouragement?
What people or problems may they have visibility into, that I don’t?
Then, when you’re ready to engage with them, send a short, friendly re-introduction. You could give a quick update on what you’ve been working on recently and any relevant updates. Share any recent article that you’ve written - or an impactful one that you’ve read. Let them know about the success of a project that you’re working on, or even a detail about someone you met that might be mutually interesting to them.
Try to make it easy for them to conceptualize you and understand you by using simple, clear language, such as, “I’m working on implementation of new AI software in my practice.” Then use your curiosity about the other person and ask them what projects they’re working on. Doing this in small pieces, week by week over time, is more impactful over the long term, than trying to chunk this all into one heroic effort at one time point during the quarter. Ultimately, see if you can trend towards bringing people together into some sort of gathering - online discussion groups, in-person dinner events, informal get-togethers that bookend conferences. These have the strongest long term impact, and over time, your network gets to understand who you are and what you stand for. When people think of you, they think of a clear idea - and the physician behind it.
Ultimately, you didn’t fail to build and maintain your network. You built one over fifteen years of training and practice without noticing - and never looked back to see what it had become. Much more than simply a favor bank held in reserve, it’s always been a living architecture of trust, credibility, and opportunity, waiting for you to see it clearly.
Once a physician begins to activate their network, the next question is how these assets compound over time. That is exactly the question that I’ll tackle in detail in the next essay. It’s about the Physician Leverage Flywheel, where knowledge, credibility, network, platform, capital, and opportunity feed one another.
Take a few minutes this week and write down a name you haven’t thought of in years. Look up what they’re doing now. Reply and tell me who came up for you - I’d love to know what you find.
Scott F. Cameron, MD is a practicing radiologist, AI implementation leader, angel investor, and MRS Past President. He writes about physician career architecture at Physician Vantage Studio.