

What AI Might Really Mean for Physician Careers
A new class of roles for physicians is emerging, shifting the career landscape, in tandem with the widening gap forming between two different physician archetypes.


I remember reading the frantic press headlines from the media coverage of the Radiological Society of North America (RSNA) Conference in 2016. Everywhere, suddenly, the sky was falling. Famously, Geoffrey Hinton proclaimed that residency programs should stop training radiologists immediately because AI would be taking over. And he compared the radiologist to Wile E. Coyote standing at the edge of a cliff and not realizing that he was about to fall off.
A decade later, the reality is that not only are radiologists very much still an integral part of the patient care journey, but they are also in very high demand in the healthcare marketplace for a variety of reasons. Nevertheless, a lot of individuals believe that Geoffrey Hinton was directionally correct, and this notion of how AI will re-shape physician careers deserves serious attention as we see how dramatic the capabilities of these technologies have become. Having said that, this isn’t a doom narrative, and it isn’t a hype narrative either.
If you’re anything like me, anytime you’re at a cocktail party and let anyone know that you’re a physician - especially if you are a radiologist - there is a greater than 50% chance that the next statement out of their mouth will be, “So what do you think about AI?” What they usually mean is, “Do you think you’ll still have a job in the next five years?” But the more useful question - and the one I’ll focus on in this essay - is, “Given that AI is the single most consequential development of our professional careers, how can we position ourselves strategically to stay relevant and come out on top? How does AI change a physician’s value?” I believe that AI is the most powerful driving force that makes complacency about your career arc dangerous, and career design very valuable. AI can certainly be used as a tool and as an agent, but it is most powerful when wielded as career leverage.
At a high-level, let’s think about the application of AI into 3 levels:
Tool usage (prompts, ambient scribes, elevated search/research, general productivity, etc)
Workflow (triage, prior-authorization, communication loops, etc)
Career Architecture (new roles and optionality, acceleration of existing forms of leverage, and access to new levels of authority)
Level 3 is what this essay is about: how AI is creating novel physician roles, accelerating certain forms of leverage, and widening the gap between physicians intentionally designing their careers around it and those who have a watch and wait perspective.
“Knowing what AI tools to use as a physician is the first step. After this, the next step is asking: what new forms of physician value, credibility, leadership, and optionality are accessible because of AI? We need to shift from tool anxiety to career architecture.”
Here’s what’s shifting right now. Firstly, AI technologies are becoming increasingly good at pattern recognition, across all domains of medicine. While imperfect, narrow use cases - such as detection of pulmonary nodules on CT scans, or patient triage, or prior authorization workflows - all of these are becoming faster, cheaper, and more seamless with AI. The gains are real, but they have been taking longer than expected and are still bounded by certain conditions that need to be true in real clinical environments. This doesn’t mean physician pattern recognition disappears, rather the value stack starts to skew towards the judgement, communication, and orchestration abilities of the physician. As this happens, the value of these human skills increases - there starts to be more of a premium placed on the ability to synthesize ambiguous data, to handle edge cases, and to communicate uncertainty to patients and other physicians.
Many AI discussions - particularly those in the C-suite - focus the conversation about AI around efficiency - more clinical work completed by fewer physicians, coupling AI with Advanced Practice Providers (APPs) to reduce the number of physicians on staff, and so on. These strategies are important value drivers, but for the purposes of this essay, I want to focus on something different.
"If we think only in terms of our current job description, and worry about AI's impact on labor replacement, we'll fail to appreciate new forms of value."
As the human-specific elements of healthcare delivery move up the value chain and AI technologies mature in tandem, we will see an increasingly wide gap develop between physicians who use AI and are AI-literate, versus those who either don’t use AI or who interact with it very passively.
Given that, here’s a suggested way to think high-level about AI. Think of it as career leverage, and not just a clinical tool. The latter is something that is given to you to use in the workflow - whether you asked for it or not - almost like something done to you or done to your practice. The former is thinking about AI as an amplifying force for the five forms of physician leverage that you already have, discussed in a prior essay. AI isn’t a new form of leverage. It’s a force that accelerates the five you already have. Let’s look more closely at each one:
Knowledge leverage: Understanding how to use AI tools in a clinical context becomes a new form of knowledge, differentiating those who are AI fluent from those who are not. This form of physician who has the technical capabilities of using AI to drive outcomes or efficiencies becomes more rare and valuable.
Credibility leverage: Becoming an early, trusted voice on AI confers a form of differentiation and leverage because most clinicians are either silent or engage with AI from a position of cautiousness or fear, or they are too busy to engage with an AI in a meaningful way.
Network leverage: AI touches so many disciplines of healthcare and innovation that it creates a meaningful way for physicians to expand their network. They can be exposed to founders, engineers, scientists, writers, investors, and others, in ways that they may not have through a routine clinical career.
Platform leverage: Given that AI is one of the hottest and most in-demand topics, a physician who speaks or writes about AI can gain a meaningfully large audience. The demand for discussion and expertise on this topic may be higher than any other.
Capital leverage: AI familiarity and expertise can translate into advisory opportunities, investment opportunities, and other ownership roles in this rapidly expanding segment of the healthcare ecosystem.
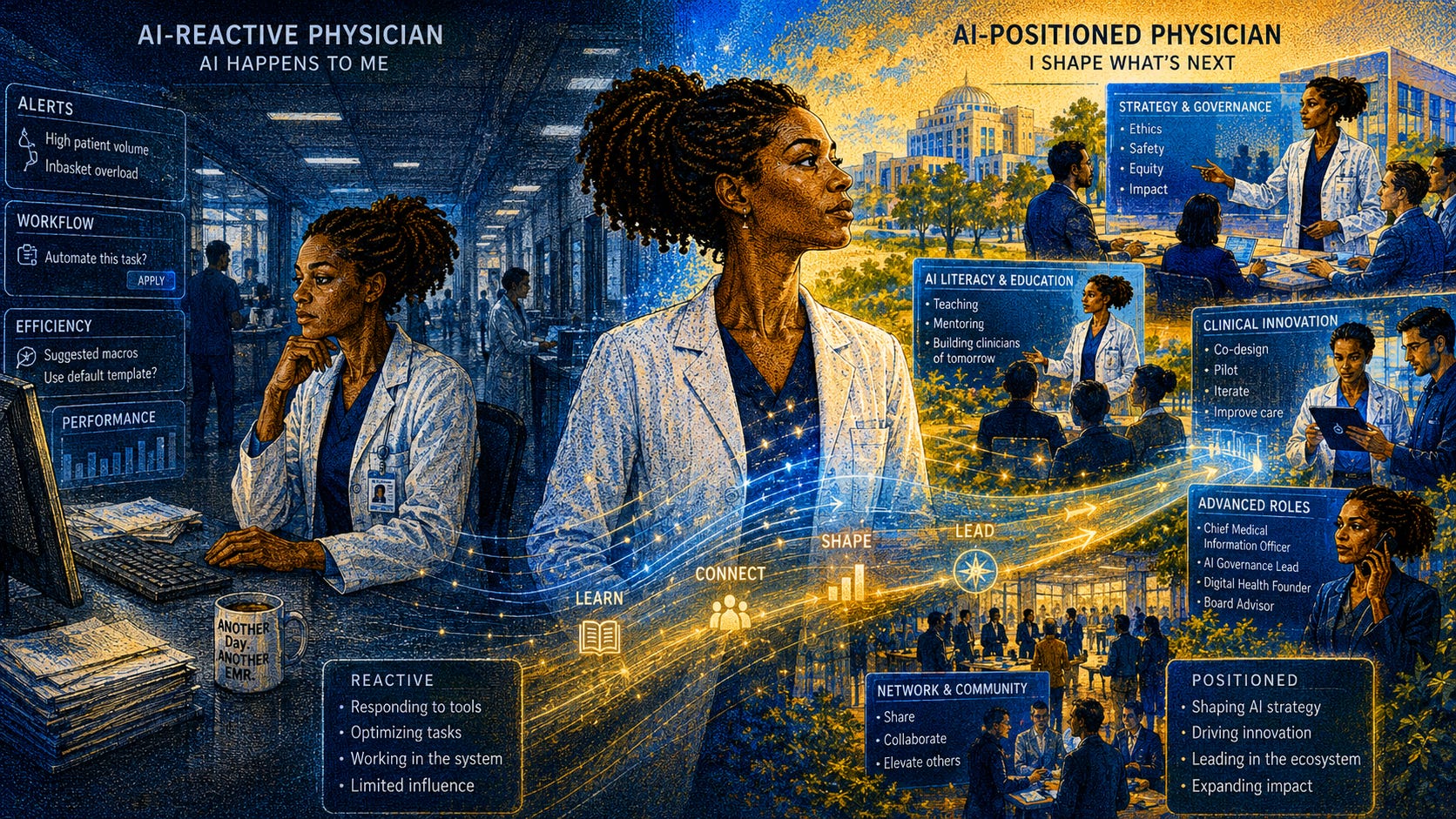
Let’s contrast two physicians - one who is AI-reactive, and one who is AI-strategic.
The AI-reactive physician is fully intelligent and capable but views AI primarily as something that is happening to them. They wait to see what AI tools will be integrated into their workflow and then they start to learn how to use them. They think about AI primarily from the lens of disruption or efficiency and their default thinking tends to drift towards “how will AI affect my job?” They like to wait to see how AI will be adopted by others in the community and others in their specialty, and when the tool is unloaded into the workflow, they learn just enough about it to maintain competence in using it. From a career standpoint, it’s ‘something happening to them’, and in a five-year time horizon they are a competent physician who is able to use the tools in the marketplace, but they are essentially interchangeable with other physicians. Their leverage position is either the same or lower than what it was five years ago.
In contrast, the AI-positioned physician thinks about AI opportunistically, strategically, and from the perspective of something that is coming and will cause disruption, but that can be harnessed for positive gains for patients and the profession. This physician thinks about how they can best use AI tools and technologies in advancing the goals of their practice. They think about what opportunities that AI will create both in their institution and outside their institution - this is AI being used as material for new roles. They view AI as an exciting way that the career is being expanded. They look at AI education and fluency as a required investment into their future, and as a way to potentially differentiate themselves from the more AI-passive physicians. They don’t just learn the minimum required to use the tools, but they look at many tools across the marketplace, trends across the industry, and develop a point of view about where things are now, and where things are going. They look for roles that let them shape AI’s direction - in the rooms where these decisions are made - rather than just receive it. On a five year time horizon, they become a respected public voice that has greater career optionality and leverage. They experience the compounding effects of knowledge, network, and platform.
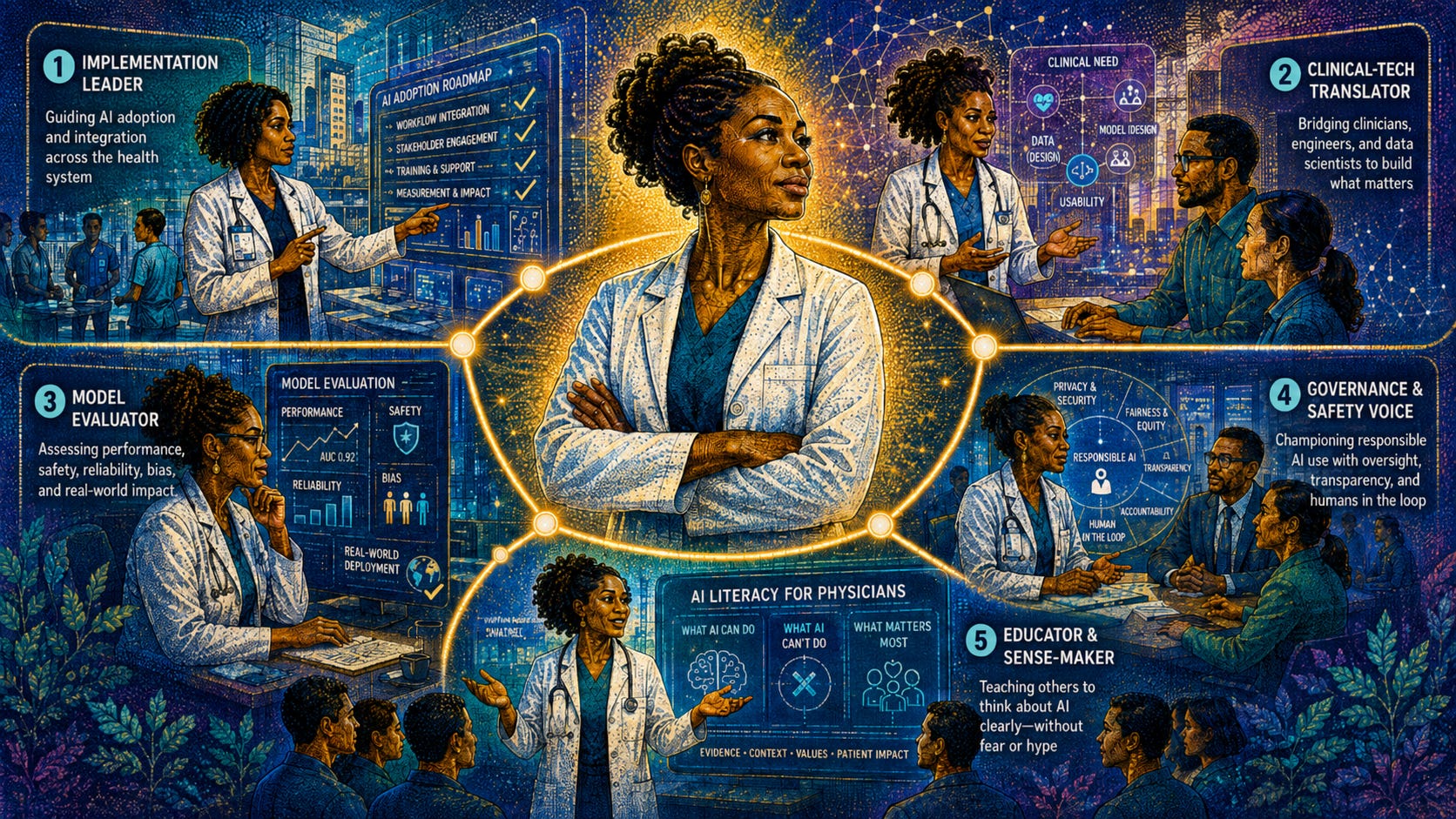
AI has already created new roles adjacent to clinical work. Here are a few practical examples which are emerging at the intersection of medicine and AI. Not every physician should pursue these, and also we should keep in mind that they can co-exist with active clinical practice. They are listed as examples to make the opportunity more specific and concrete:
The implementation leader guides AI evaluation and adoption inside a practice or healthcare system - understanding not just the technology but the clinical use cases, the true clinical workflow, trust dynamics and buy-in, and how clinicians actually behave when new tools hit production.
The clinical-tech translator helps engineers, data scientists, founders, and physicians understand each other. Clinical expertise informs product and process requirements that developers don’t necessarily possess on their own.
The model evaluator assesses AI tools from a clinician’s perspective - performance, safety, usability, brittleness, real-world reliability, data bias and drift - helping bridge the gap between a promising demo and successful real-world deployment.
The governance and safety voice participates in oversight, policy, and risk evaluation for responsible AI deployment. This is the physician or clinical champion who makes sure that the humans stay in the loop.
And the educator and sense-maker teaches other physicians how to think about AI without resorting to tips, fear, or hype - a role that is increasingly needed and more underserved than most others right now.
Again, none of these require abandoning clinical work wholesale or joining a startup. For most physicians these start with one decision and one action.
"Think of AI as the wave of technology that spawns new physician roles for those who can combine clinical credibility, judgment, translation, communication, and implementation."
In my own professional work, I’ve walked down some of this road. Having been interested in AI for many years, particularly in the specialty of radiology, which lends itself very well to many AI applications, I started to learn early on about different AI companies and the tools they were developing. This included companies like RadAI (in which I later became an investor, disclosed below), developing tools to streamline radiologist reporting and closing patient communication gaps, and Prenuvo, developing whole-body MRI screening technology. This led me to being more deliberate about my AI education, and I completed the Radiological Society of North America (RSNA) Imaging AI Certificate Program. This course taught me how to assess and confidently use AI tools, and the different parts in the development of AI algorithms. After the course I felt more comfortable in knowing how to safely evaluate, deploy, and monitor AI tools in my practice. This doesn’t mean I became an AI expert, rather, it gave me the baseline knowledge where I felt comfortable being in the rooms where discussions about AI are had. In my practice - and in many others out there - that is relatively rare.
This then informed the evaluation, selection, and usage of some software we then used in our practice, such as Koios AI for thyroid nodule detection. Today, I sit on the Optum AI Advisory Board, where we critically evaluate emerging AI technologies and platforms and their potential benefit across multiple Care Delivery Organizations in our network. In this capacity, I see where there’s hype and where there’s reality - the potential gap between the demo and the deployment. This is practical, real-world knowledge that makes a difference in how healthcare is delivered.
Along the way I also started to learn - through my network - about opportunities to participate in AI imaging trials. These studies helped commercial vendors creating AI algorithms for radiology applications understand how the software would work in radiology applications. Through these trials, supporting companies such as ContextFlow, Aidence, and IBM Watson Health, I participated as a reader and helped evaluate new artificial intelligence software algorithms in the diagnosis and characterization of lung nodules on chest CT scans, the detection and diagnosis of liver disease, and other applications.
At around the same time I also became involved in AI as it touches the investing domain - I became a clinical advisory board member for AngelMD, as well as a member and investor of Launchpad Venture Group. Through these activities I joined a group of early-stage startup investors in evaluating rapid-growth startups that were aimed at creating innovations in healthcare (as well as non-healthcare sectors), many of whom were using AI - one such company that came across my radar was the aforementioned RadAI. Through evaluating these startups, I get a glimpse into the problems these founders are trying to solve, and the physician-centric elements that they can’t replicate.
This isn’t to say that you need to do all of these things in order to parlay your interest in AI into larger opportunities - the point is the orientation around how to approach AI and how to participate in ways above and beyond simply using AI technologies once they are integrated into your practice - and wondering ‘What’s going to happen to me?’

The certificate I earned started with one course.
The investing started with curiosity.
The advising started with one conversation.
Each led to the other.
Ultimately, AI is here and is accelerating change in all industries - with healthcare being no exception - but the real frame here is AI as career leverage. There are real challenges, questions, and limitations around how these technologies will be able to be used in clinical workflows. The time to engage with it and be proactive is here, and it’s available to any physician, regardless of specialty, background, or skillset. It’s possible to engage in a way that matches your interests and aptitude and fits within the context of who you are professionally and how you practice - every specialty has it’s AI-adjacent frontier. This isn’t a call to become a data scientist, an engineer, or a machine learning expert. After all, as discussed previously, it’s the human judgement, coordination, and communication layered on top of the AI-augmented intelligence that will drive value. This physician-anchor remains foundational as you build AI-fluency across your career - and remember that this shouldn’t be viewed necessarily as a new task, but rather a new lens that makes your work more leveraged.
For a next step, think about where it is in your clinical practice that you already have specific credibility? What AI-adjacent clinical problem do you understand better than most of your colleagues - and what role could you test out, in a small way, in the next 90 days?
My belief is this: AI won’t end the physician’s career. It will end the AI-reactive one.
If pure diagnostic ability and pattern recognition starts to decline in value, then the physician who builds beyond that - by developing their integration, communication, AI-fluency skills, and different forms of leverage - will start to become the de facto ideally positioned physician. This means that the natural form of the physician role won’t be the conventional standard ‘one job, one role’ but rather a portfolio. There’s a name for the type of career that fits this moment in time, that is crafted with multiple deliberate layers rather than in a single track. I’ll be writing about that next.
Where are you in your AI journey currently? Thinking, exploring, using, building, worrying…? Using AI as a clinical tool in your practice, or as something that you’re actively building with, as leverage? Let me know in the comments.
Disclosure: I hold investment positions in and advise healthcare AI companies, including RadAI and through Launchpad Venture Group and AngelMD. I also participate in AI evaluation work in my clinical role. The views here are my own, are not intended as an endorsement of any specific company, and are not those of my employer or any affiliated organization.
Scott F. Cameron, MD is a practicing radiologist, AI implementation leader, angel investor, and MRS Past President. He writes about physician career architecture at Physician Vantage Studio.