

The Default Physician Career Script

I remember one quiet morning walking into my office and cleaning off my keyboard, turning on my monitors and the lamp behind them, and sitting down and staring at an incredibly long list of imaging cases for me to read. I realized in that moment that this was deja-vu all over again from last Tuesday and the Tuesday before that. I understood that I was essentially executing the same plan over and over again, with no real reflection on where it was ultimately going. I was essentially doing my job - and I felt a sense of predictability, not possibility. Most physicians have never written a career plan. Rather, they have followed a path, but a path is not the same thing as a plan. I had been executing someone else’s design of a career. And the more I looked around, the more I realized almost every physician I knew was doing the same thing.
I was executing a default physician career script. I was living in it.
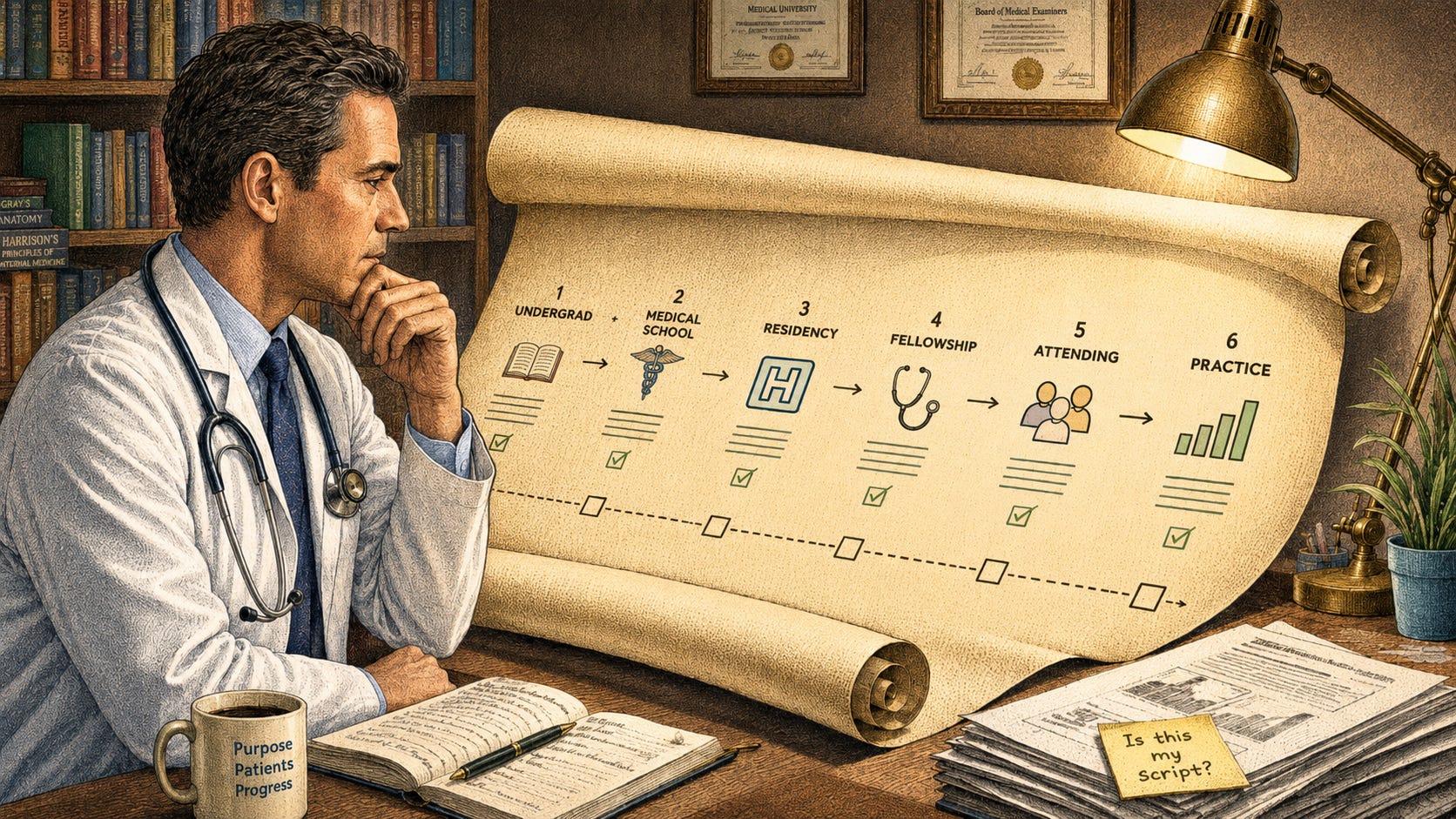
Here’s how I break down the Default Physician Career Script:
Stage 1: Pre-med: Make sure you have the highest grades possible. Volunteer in a hospital or health clinic if possible. Shadow a physician. Perform well on your MCATs. Ultimately decide you want to go into medicine by your late teens or early 20s before you have any significant meaningful exposure to medical practice.
Stage 2: Medical School: Intense focus on didactic courses and dedication to core clerkships. Decide on a specialty based on perceived interest, lifestyle, prestige, salary, or the random influence of one or two friendly or charismatic attendings.
Stage 3: Residency: 50 to 80 hour work weeks. Overnight shifts. Submission to hierarchy. Making a fellowship decision based on the fact that “everyone successful in this specialty does a fellowship”.
Stage 4: First Attending Job: Choices made based on geography, where a partner works, proximity to family members, or whichever practice made the first reasonable offer.
Stage 5: Mid-career: Productivity expectations, RVU metrics, committee responsibilities, slow accumulation of administrative burden, the same Tuesday in clinic year after year. Seeking titles, partnership, leadership.
Stage 6: Pre-retirement: Decrease hours to part-time. Mentor the next generation of physicians. Retire. The end of the default career script.
At no point in the path does someone necessarily stop you to ask, is this what you actually want?
This script isn’t necessarily a bad thing, or even bad intentioned. It’s created by structural forces that individually make sense and to keep you progressing along the path.
This script gives physicians a clear path, external validation, stable income, a sense of professional and social respect and identity, and deep clinical expertise. However, the script doesn’t necessarily give you insight into how to design a second professional arc, how to utilize leverage beyond your clinical productivity, how to negotiate or create roles, how to assess optionality, or how to choose a path when no one guides you towards the next step.
It’s easy for physicians to stay on this path because from the very outset we know that medicine attracts and awards individuals that are excellent at executing well-defined paths. We’re very good at learning what the next step is in the chain and preparing ourselves and doing that very well. Consider the pre-med student who mapped out every prerequisite and extracurricular activity, and every shadowing opportunity - not because anyone told them to, but because those are the next steps required. Medicine selects for exactly that skill: executing a well-defined path with precision and discipline. Furthermore, during the course of either education, training, or practice, things can be so busy and time can be so scarce that there’s very little bandwidth to think about and consider other career alternatives or paths. A specialist may want to write publicly to clarify their ideas and create unexpected opportunities, but may not necessarily have the time in their schedule to do so.
By the time the bandwidth appears in mid-career, the script has started to feel normal. Not chosen - just normal. And there’s a meaningful difference between the two.
Your training path is over, but your professional life is not. The rewards that are coming to you can be some variation of the same. More volume, more responsibility, more titles and committees. You may have more credibility, but not yet have the language for using that credibility in a different way.
Furthermore, when everyone around you is following the same path and executing the same script, alternatives can feel somewhat illegitimate. Lastly, financial pressures can create a sense of commitment to the path that financially sustains you.
While these things all make sense, we have to consider that there is a hidden cost here. One cost is lost optionality. Understanding that decisions that are made at an early age, such as age 24, when you make your specialty choice, can constrain your options down the line when you’re 44. This impacts your career architecture. This script essentially forecloses possibilities that you didn’t know existed. The more that you invest time into this path, the more calcified your identity becomes and the harder any deviation from that becomes.
A second cost is identity fragility. When your professional identity is built on one script, anything that threatens it can feel like a threat to who you are. AI changing your workflow feels existential. A difficult year feels like a crisis of the self rather than a difficult year. The narrower the identity, the more fragile it becomes.
The third cost is harder to name but easier to feel. It’s the quiet discovery - often in mid-career, often on a Tuesday morning - that the script delivered exactly what it said it would. But what it promised isn’t actually what you wanted. The script succeeded - but the question is whether it succeeded at the right thing.
The script did exactly what it was designed to do. The question is whether it was designed for you - or designed by you.
The problem which most physicians intuitively realize is that even if you wanted to follow this script for the next 20 years, there are accelerating external forces that are making it harder to do so and that are threatening to break this model. This script was designed for a world and an environment that no longer exists. One huge disruptor is AI and workflow changes. And we know that the way physicians are performing their work is changing faster than the script can adapt to. We understand that AI literacy is becoming a career asset and may eventually become a requisite, but it’s not part of the default career script. Another driver is productivity pressures and reimbursement declines. The economics to sustain a clinical practice are becoming increasingly strained. Pure clinical careers are becoming financially less rewarding, adjusted for the amount of work input relative to the alternatives. Healthcare consolidation and the rise of employed physician models have reduced the autonomy the default script assumed. We have to understand that designing our own career architecture is no longer a luxury, but rather a necessity. It’s a shift for the world physicians are actually operating in.
The good news is that there is a possibility around the corner to address this Physician Optionality Problem. While we understand that there is a script executor who essentially follows the default path, reacts to situations and opportunities as they arise, and measures success by external metrics, we also understand that there is an alternative. The alternative isn’t dramatic reinvention. It’s a different orientation to the same career. For example, you can be a clinician negotiating an AI implementation role within your institution. Or you can be a physician using advisory work, consulting, or teaching as an expansion layer as opposed to an escape pathway. The metric shifts towards intrinsic variables where success is measured against the barometer of alignment with your actual capabilities, skills, values, and interests.
Intentional physician career design and physician career architecture is all about asking different questions.
It’s not necessarily what’s the next step for me, but rather: what do I want to be building or creating over the next ten years?
Rather than asking what opportunity should I accept, ask: what opportunity should I create?
The question is not necessarily should I be clinical or non-clinical? It can instead be: should I follow an inherited path or an intentionally designed path?
This shift in perspective can generate a meaningfully different career.
The default physician career script was created for the average physician in 1996. You are not the average physician, and this is not 1996.
We should operate from a vantage point of physician evolution, not revolution. Your clinical skills and experience serve as your foundation, not as a constraint.

This is the progression we’ll be building out across the coming essays — starting with why Identity Compression makes the first move so hard.
In the next essay, we’ll take one specific driver of the Physician Optionality Problem -Identity Compression - and dive deep. Identity Compression is the deepest reason physicians stay stuck, and recognizing it is the first step toward redesigning it.
If this essay resonates with you, let me know. Which stage of the script hits hardest for you?
- Scott F. Cameron, MD
Radiologist. AI implementation leader. Angel investor. MRS Past President. Career architect.